For decades, research into Alzheimer’s disease has centred on neurons. Only in the past few years have scientists identified a role for immune cells in the progression of this neurodegenerative disorder1. Most research has focused on the nonspecific, innate branch of the immune system. But writing in Nature, Gate et al.2 report that an immune-cell subpopulation belonging to the adaptive immune system — which remembers and responds to specific foreign invaders — might also have a role in Alzheimer’s disease.
The authors isolated and analysed immune cells from the blood of healthy people and people who had Alzheimer’s disease or a precursor of the disease known as mild cognitive impairment (MCI). They discovered an immune-cell subpopulation called CD8+ T effector memory CD45RA+ (TEMRA) cells that was associated with MCI and Alzheimer’s disease. TEMRA cells have previously been linked to immunological memory, and they release inflammatory and cytotoxic (cell-death-promoting) molecules3.
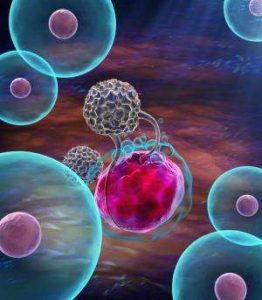
Analysis of a separate cohort of people who had Alzheimer’s disease revealed that an increased presence of TEMRA cells in the blood was associated with compromised cognitive performance. This finding could indicate that TEMRA cells contribute to neuronal dysfunction by secreting inflammatory and cytotoxic molecules in the brain (Fig. 1). Alternatively, a damaging mechanism that causes cognitive dysfunction might also elicit an inflammatory TEMRA-cell response in the blood.
Gate et al. corroborated their findings in vitro, showing that stimulation with an inflammatory molecule caused immune cells from people who had MCI or Alzheimer’s disease to release more interferon-γ (a key pro-inflammatory protein) than did immune cells from people who did not have these conditions. This is consistent with another study4, which demonstrated that T cells derived from people who have Alzheimer’s disease become more active than do those from healthy people when exposed to β-amyloid, a protein associated with this disorder.
The authors then asked whether the presence of TEMRA cells could be used to predict disease status. Indeed, a machine-learning algorithm could use measurements of TEMRA cells (together with information about other immune-cell populations) to distinguish between healthy people and those with MCI or Alzheimer’s disease with about 80% accuracy. Many immune processes alter during ageing and so are of limited use for predictive clinical testing, but age did not influence the level of TEMRA cells. This type of technique, once refined, might therefore be used alongside biomarkers of neuronal damage and degeneration for blood-based diagnostic tests, improving our ability to detect Alzheimer’s disease at an early stage.
Next, Gate and colleagues analysed the brains of people who had died with Alzheimer’s disease. This revealed CD8+ T cells (which might be TEMRA cells) in the perivascular space around the brain’s blood vessels, and at sites of β-amyloid deposition, as previously reported for T cells in Alzheimer’s disease5,6. CD8+ T cells are known to physically contact and sever neuronal processes, causing structures called neuritic spheroids to form nearby — another hallmark of Alzheimer’s disease7. Thus, it is conceivable that TEMRA cells contribute to neuronal damage not only by secreting immune molecules, but also by directly damaging neuronal processes7.
MCI and Alzheimer’s disease are associated with changes in the number and proportion of T cells in the cerebrospinal fluid (CSF) that surrounds the brain and spinal cord8,9. The investigators therefore asked whether TEMRA cells were found in the CSF and whether there was evidence of ‘clonal expansion’ of this cellular subpopulation. Naive T cells each have different T cell receptor (TCR) proteins, but when the receptor is stimulated by a particle called an antigen, the cell proliferates to form clones of itself. The presence of more than one cell with the same TCR therefore indicates clonal expansion — a sign that T cells have been activated previously. The authors sequenced TCRs from an independent cohort of people and identified several T-cell clones, including TEMRA cells, in people with Alzheimer’s disease. This is perhaps the first evidence that clonally expanded T cells invade the CSF in age-related neurodegenerative diseases.
Gate et al. then validated their result using gene-expression analysis. This revealed that the TEMRA-cell population was the predominantly expanded T-cell clone in each person who had Alzheimer’s disease. The population expressed various cytotoxic genes, and was enriched in the hippocampus — a brain region crucial for human memory. In line with this observation, hippocampal T-cell infiltration promotes cognitive decline in a mouse model of Alzheimer’s disease10. The authors also found evidence for TEMRA-cell clones and gene-expression changes in the CSF of people who had another neurodegenerative disorder, Parkinson’s disease, highlighting the possibility that different age-related neurodegenerative diseases share similar molecular underpinnings.
Which antigens drive clonal expansion of TEMRA cells? By comparing TCR sequences from people who had MCI and Alzheimer’s disease, the investigators found evidence that clonally expanded TEMRA cells had been bound by two antigens produced by a virus of the herpes family, Epstein–Barr virus (EBV). However, it is important to note that a role for EBV infection in neurodegeneration has not yet been reported, and Gate et al. make no suggestion that EBV is involved in the development of Alzheimer’s disease.
Gate and colleagues’ data involve only a few patients and should be interpreted with great care, particularly given that EBV infects about 95% of people during early life11. Previous work12 has shown a complex relationship between herpes viruses and Alzheimer’s disease in mice. One the one hand, β-amyloid fibres can entrap herpes viruses, extending survival in mouse models of Alzheimer’s disease. But on the other hand, virus infection strongly increases β-amyloid deposition in these animals.
In addition, a study11 of 85 people who had Alzheimer’s disease found evidence of EBV DNA in the brains of only 6% of cases. All of these people carried the gene APOE4, which is associated with a high risk of Alzheimer’s disease and could explain why they developed the disorder. The same study did find that antibody responses against EBV increased during cognitive deterioration and progression of Alzheimer’s disease11. However, these responses are quite common in older people. Moreover, a recent meta-analysis found no correlation between herpes-virus infection and dementia13. Longitudinal studies involving many more people will be needed before solid conclusions can be drawn.
It will be interesting to reconcile Gate and colleagues’ data with the finding14 that T cells can restrain cognitive deficits in mouse models of Alzheimer’s disease. Analysis of less-prominent T-cell clones in people with and without disease might reveal other, potentially harmful — or even protective — subclones. In addition, the current study will no doubt renew efforts to define the crosstalk between innate and adaptive immunity in general, as well as in neurodegeneration. Perhaps, in the future, these interactions could be harnessed for diagnostic purposes or to develop therapeutic interventions.